The role of the doctor as a healer is an ancient calling as old as humanity itself. Human skeletons dating back to 6500 BCE bear evidence of medical interventions, including, remarkably, brain surgery [1]. Yet modern medicine is far younger. The rise of evidence-based medicine has transformed healthcare over the past century. The next transformation will come from harnessing medicine’s information flows to build increasingly autonomous healthcare systems. But healthcare is only one part of a much broader societal system. Since this more of a mystery to solve than a curriculum of ideas, let us begin where every good scientific investigation starts: first principles.
What Is Healthcare?
Healthcare has always been fundamental to humanity. Most other industries and systems - from financial markets to green technology - are simply emergent properties of scale. Keep this in mind, because it becomes important when considering healthcare’s wider effects.
The fundamental aim of medicine is to use knowledge to reduce suffering, reflecting our evolutionary wiring to preserve and improve human life. Healthier populations are better able to contribute to and advance society. But why must humanity continue to progress? Because standing still is rarely neutral; it is often regression. Civilizations either advance or decline - rarely there is steady state. History reminds us of this: the Egyptians lost the knowledge behind pyramid construction, while the Romans lost much of the expertise behind aqueduct systems - limiting their societies’ ability to progress and adapt, and arguably contributing to their eventual collapse. Healthcare is ultimately an investment in humanity’s future.
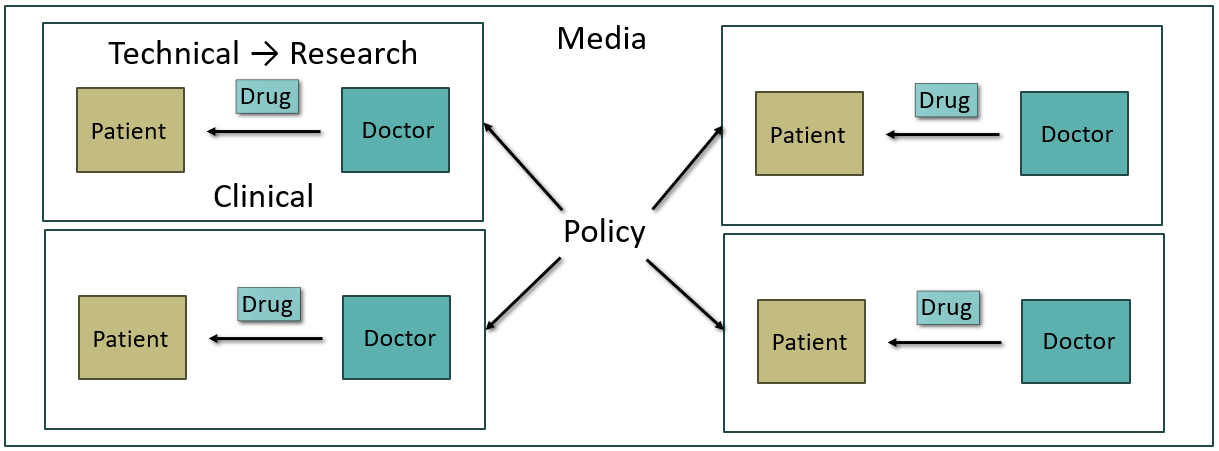
Consider a patient who is ill. Medicine’s immediate goal is to restore their health. A doctor delivers care (clinical pathway). But doctors rely on tools and therapies developed by engineers and biologists (technical pathway). These tools improve over time, driven by scientists, academics, and clinical researchers (research pathway). To deploy healthcare effectively across entire populations requires complex coordination (policy pathway). Finally, knowledge must flow between all entites so better decisions can be made over time (media pathway).
Together, these pathways extend medicine beyond the doctor–patient interaction to form a healthcare system.
The Future of the Doctor
The future doctor will do more than treat patients - they will build the systems that treat patients. This shift is subtle but profound. Instead of improving one consultation at a time, they will create solutions that improve millions. Scale becomes the force multiplier.
The next generation of healthcare leaders will not rely on clinical medicine alone. They will combine medicine with at least one additional pathway from our first-principles framework: technical, media, research, or policy. Each comes with different incentives:
- Technical → creating value
- Media → spreading ideas
- Research → advancing knowledge
- Policy → shaping systems
Technical and media pathways offer exceptional leverage because digital tools and information can be replicated at near-zero marginal costs and scale globally. While building software or an audience requires significant effort, a single product or idea can reach millions - far beyond the impact of any individual clinician. This is why doctors such as Ali Abdaal have explored careers beyond traditional clinical practice.
Information itself has become one of humanity’s most powerful assets. For thousands of years, from early manuscripts (~3000 BCE) to books, knowledge spread slowly amongst the elites limited by high costs of manual replication. The printing press democratised access in 1440, while the internet reduced the marginal cost of replication to zero following the creation of the World Wide Web in 1991. As information became easier to replicate and distribute, its ability to shape society increases dramatically across all industries. Healthcare is no exception.
Research and policy remain equally important, but face distinct incentive structures. Research advances medicine, yet modern academia often operates within a publication–grant flywheel that can prioritise output over discovery. Policy can transform healthcare at national scale, but political incentives, short-time horizons, and asymmetric information make meaningful reform difficult.
In practice, these pathways are surprisingly accessible:
- Technical - learn to code and solve problems.
- Media - write, teach, or create content.
- Research - join a laboratory or research group.
- Policy - contribute through public health and health policy, including specialties such as Public Health Medicine [2]
There is no single optimal path. A powerful strategy is to build permissionless leverage first through technical and/or media pathways. Research can generate evidence and strengthen credibility, while policy becomes most effective after demonstrating execution ability.
Ultimately, the doctor’s role is not simply to practise medicine, but to find new ways to use knowledge to reduce suffering. Clinical medicine is the foundation, not the destination; being a doctor is the floor, not the ceiling. Rather than choosing one of 65 specialties and remaining within its boundaries, future doctors will combine disciplines to create careers uniquely suited to the problems they want to solve [3]. These pathways do not offer a fixed blueprint, and are often percieved as ‘risky’, but they maximise optionality - allowing unexpected opportunities to emerge from the intersection of knowledge, networks, and technology. The future belongs to doctors who embrace this convergence and use it to build systems that improve health at unprecedented scale.
Solving Health
“Young men die of accidents, middle-aged men of disease, and old men of age.” - Aristotle
Aristotle’s aphorism provides a useful framework for thinking about the future of healthcare. Nearly every major innovation ultimately targets one of three goals:
- Autonomous healthcare systems - software, AI, and robotics
- Curing all disease - intelligent scientific discovery
- Reversing aging - biological rejuvenation
These goals may sound impossibly ambitious, but they are better viewed as asymptotes than destinations. We may never fully reach them, yet every step towards them improves human health. The important question is not to debate whether they are possible, but how we can accelerate progress towards them.
Reversing ageing illustrates this well. A decade ago, the elusive “fountain of youth” belonged largely to science fiction; today it is a serious area of scientific inquiry. As knowledge compounds, ideas once thought impossible become increasingly plausible; the boundary of possibility is not set by today’s technology, but by the laws of physics.
Yet some secrets may best be left undiscovered. Technologies that are extraordinarily difficult to create can become extraordinarily easy to weaponise. Every breakthrough carries consequences beyond medicine. Extending lifespan could reshape society in unintended ways - concentrating wealth and power, slowing generational renewal, and risking the ossification of civilisation, where fewer new ideas emerge, yielding dystopian outcomes. At the extreme, such technologies could destabilise global security. If we do indeed live in a simulation, perhaps death is not a flaw to be eliminated, but a feature that drives renewal, innovation, and the continual advancement of humanity.
Even if we eliminated accidents, disease, and ageing, one challenge would remain: human flourishing.
“Many people die at 25 and aren’t buried until they are 75." - Benjamin Franklin [4]
- Human flourishment - information
Health is more than the absence of disease. It is the ability to live a meaningful, purposeful life.
Purpose is paramount. Without a compelling direction, many people default to safe, conventional paths that fail to fully realise their unique talents - arguably the worst thing a person can do with their life. The result is not merely reduced productivity, but diminished wellbeing. The human brain is designed to solve meaningful problems, and a life without purpose carries psychological costs that medicine alone cannot treat.
However, progress is being made. AI-enabled universal basic income and creators such as Simon Squibb are challenging conventional beliefs and encouraging deeper reflection on purpose. Yet lasting solutions will require more than technology alone; they will emerge from collaboration across disciplines, where ideas combine to solve problems no single field could address alone.
A deeper consideration is that the most powerful people in society are not politicians or billionaires, but the engineers designing social media algorithms that shape what billions see each day. Information shapes attention, behaviour, and ultimately health - affecting what people eat, how they think, how they spend their time, and even who they elect. Healthcare therefore cannot be separated from the wider information ecosystem. The antidote to chaos would be empowering people with greater control over the information they consume. This is tough but should be possible.
Ultimately, healthcare is not just about extending life, but improving its quality. Solving health may unlock solutions to downstream societal challenges - including crime, addiction, lust - bringing us closer to a more utopian society.
The First Frontier: Autonomous Healthcare
Healthcare systems exist to reduce suffering through effective treatment, but scale creates unavoidable trade-offs with current models. Three constraints define the challenge:
- Effectiveness - the quality and reliability of care
- Speed - how quickly patients receive appropriate treatment
- Affordability - the cost of access
Most systems optimise for only two:
- Free systems (e.g. UK) → effective and affordable, but slower access
- Private systems (e.g. US) → effective and fast, but expensive
- Hybrid systems (e.g. India) → fast and affordable, but less consistently effective
![]()
The question is whether all three can be achieved simultaneously. Advances in software and AI create a new possibility: a fully autonomous healthcare system.
The core question becomes:
Can we reduce uncertainty in clinical decision-making to the point where AI systems can consistently match or exceed human doctors?
A useful comparison is autonomous driving. Despite over $100 billion in investment and more than a decade of progress, fully self-driving cars are still not widely deployed. The key barrier is not capability alone, but safety: error rates must fall far below human levels, as even rare failures influence public trust and regulation.
Healthcare will likely follow a similar path. AI systems must demonstrate not only competence, but exceptional reliability before full integration becomes acceptable. Even then, adoption will advance one cautious step at a time due to cultural and institutional constraints.
Human-in-the-loop systems are an important transitional stage, but they do not remove the fundamental bottleneck: human time. The next generation of healthcare systems is therefore about creating infrastructure that enables increasingly autonomous decision-making.
Just as a single AI tool can now replace a skyscraper of software engineers, an integrated AI ecosystem could one day transform the role of entire hospitals. However, reaching this future is not purely a technical challenge - it will also depend on risk tolerance, regulation, and behavioural economics. Societies must continuously balance health risks against financial and systemic risks; today, in some systems such as the US, patients already avoid necessary care due to cost concerns.
This future may still seem distant, but technological progress is accelerating at an accelerating rate. AI is driving the cost of knowledge towards zero, already achieving high performance on medical exams such as the USMLE [5], while advances in robotics and physical AI continue to expand what is possible. The question is therefore not whether this transition will occur, but when [6].
History shows that transformative technologies often begin with scepticism. When CT scanners were introduced in the 1970s, they were considered experimental and raised concerns about accuracy and radiation exposure [7]. Over time, they became foundational to modern medicine. AI will likely follow a similar trajectory.
A contemporary analogy is banking: an essential, highly regulated industry dominated by large institutions. In the 1990s, banking relied heavily on paper and physical branches; the rise of smartphones and digital banking transformed it into a largely paperless system. Healthcare is more complex because it is inherently physical, but it may similarly require fewer routine human interactions. Personalised healthcare and continuous monitoring demonstrate early progress, yet siloed systems and large-scale data fragmentation remain major barriers to achieving the level of integration seen in modern banking.
These shifts imply a fundamental change in medical education and clinical training. As healthcare systems scale, costs can change non-linearly: treating 10,000 patients does not necessarily require ten times the resources of treating 1,000. With the compounding advantages of software, AI, and data, marginal costs may eventually approach zero, enabling universal access to high-quality care.
In the short term, however, a two-tier system is likely: AI-augmented care alongside traditional care, before full democratisation becomes possible. This transition mirrors the shift from bespoke tailoring to mass-produced clothing in the 1850s. Early industrial products were lower quality than tailored garments but far more accessible; over time, quality improved while accessibility remained. Healthcare may follow a similar trajectory - first expanding access through imperfect systems, then converging towards both high quality and universal availability.
The Cost of Inaction
An autonomous healthcare system represents one possible endgame for medicine. Without it, the more likely outcome is a persistent two-tier system.
What is often described as the “privatisation of the NHS” is, in practice, a structural response to rising costs and demand. As treatments become more advanced - and therefore more expensive - healthcare systems must ration access in different ways. The US represents one extreme of this trade-off, prioritising speed and innovation at the expense of affordability, while the UK prioritises universality but faces growing pressure on capacity and access. Over time, this risks widening the gap between those who can access cutting-edge care and those who cannot.
Without a breakthrough innovation, humanity risks missing out on transformative medical progress. Instead, society may continue to advance incrementally while becoming increasingly stratified by access, quality, and speed. The consequence is not merely inefficiency, but a cataclysmic inequality between those who benefit from medical progress and those left behind.
A Vision for the Future
The NHS lacks a clear long-term vision, a challenge common in large public institutions. Compared with similarly sized private companies such as Amazon or Starbucks, where cohesive strategy and rapid execution enable faster innovation cycles, public systems often face misaligned incentives, fragmented communication, and slower decision-making. As a result, the frontier of healthcare innovation is more likely to emerge in high-risk, high-execution ecosystems such as Silicon Valley.
Health has always been fundamental to humanity; everything else depends on it. A more autonomous healthcare system would not only transform medicine, but unite society around a shared goal: reducing suffering. By aligning incentives, overcoming fragmentation, and enabling coordination at scale, it could become a foundational force for a new era of human progress.
Notes
[1] Faria MA. Neolithic trepanation decoded- A unifying hypothesis: Has the mystery as to why primitive surgeons performed cranial surgery been solved?. Surg Neurol Int. 2015;6:72. Published 2015 May 7. https://doi.org/doi:10.4103/2152-7806.156634
[2] My Director of Studies at Cambridge encouraged me to consider pursuing a role such as Health Secretary. However, I believe technology will be the greater driver of healthcare transformation over the coming decades, with policy playing a more enabling and stabilising role.
[3] As Academic Officer of the Cambridge Clinical Students’ Society, I aim to encourage lateral thinking about medical careers and less siloing on traditional pathways. As the world changes, impact will increasingly come from interdisciplinary and non-linear paths - reinforcing the idea that “medicine is the floor, not the ceiling”. More thoughts here: https://karthikprabhu.me/notes/creatingvalueinhealthcare/
Historically at Cambridge, the highest-performing pre-clinical student was reportedly discouraged from progressing into medicine, based on the belief that humanity would gain orders-of-magnitude greater value from their scientific contributions than from conventional clinical practice. While this no longer applies (mainly for legal reasons), the underlying principle remains relevant: research and technology can create impact far beyond the limits of individual clinical practice.
[4] Widely misattributed, although similar versions appear in other sources.
[5] Vishwanath, K., Alyakin, A., Ghosh, M. et al. General-purpose large language models outperform specialized clinical AI tools on medical benchmarks. Nat Med (2026). https://doi.org/10.1038/s41591-026-04431-5
[6] The NHS is unlikely to transform rapidly. The frontier of healthcare innovation will likely emerge in high-velocity ecosystems such as Silicon Valley before being gradually adopted and scaled within institutional systems such as the NHS.
[7] G. N. Hounsfield, Computerized transverse axial scanning (tomography): Part 1. Description of system, British Journal of Radiology, Volume 46, Issue 552, 1 December 1973, Pages 1016–1022
Thanks to the Cambridge ecosystem for shaping my thinking through placements, supervisions, conferences, speaker events, and conversations. This includes peers across colleges and disciplines, doctors, patients, healthcare leaders, policymakers, researchers, entrepreneurs, investors, and Nobel laureates. Interdisciplinary thinking is essential; truth is rarely found in isolation, but emerges from the combination of diverse perspectives around us.